Worldwide, millions of women currently wish to delay or prevent another pregnancy, yet do not use contraceptives. Reasons for non-use of contraception are multi-faceted and complex, involving social, cultural and economic barriers, fears about side effects, and lack of access to a trusted provider.
Given the linkages between family planning (FP) and the achievement of several Millennium Development Goals related to maternal and child health and survival (along with other socio-economic development goals), the 2012 FP Summit in London sought to galvanize efforts to give an additional 120 million women and girls access to contraception around the world. Independently, USAID led an interagency process to synthesize and disseminate High Impact Practices (HIPs) to strengthen FP programs. Two categories of HIPs exist: those practices related to service delivery, and those related to creating an enabling environment.
Strategic Approach
MCHIP positioned FP within maternal, newborn and child health (MNCH), emphasizing the many health benefits of FP for mothers and children. Those benefits accrue from ensuring healthy timing and spacing of pregnancies and the fulfillment of reproductive health goals for family size. The Program’s strategy was to integrate FP within a continuum of MNCH care and services, thus reducing maternal, infant and child mortality and morbidity, averting unintended pregnancies, and achieving healthy pregnancy spacing. Ultimately, the strategy aimed to address the unique needs of postpartum women for information about timing of return to fertility and contraceptive options.
While field-supported country programs may implement more general FP activities, MCHIP’s global leadership efforts were more specific—to gather the evidence, build consensus, advocate and innovate around postpartum FP. Multi-country analyses of demographic and health survey data shined a light on a high proportion of closely spaced births, despite high responses regarding the desire to space or limit pregnancies for at least two years. Furthermore, MCHIP learned that awareness, perceptions and social norms about postpartum return to fertility and resumption of sexual activity present a major barrier to the provision and uptake of FP.
MCHIP’s approach took advantage of the frequent contacts women have with health care providers during pregnancy and in the two years subsequent to giving birth, by integrating FP counseling and services during these contacts where feasible. MCHIP-FP defined postpartum FP (PPFP) as the safe initiation of an effective method of contraception prior to the return to fertility and continuing to use a method for at least two years after a birth.
To promote PPFP, MCHIP:
- Assured proactive counseling to inform women of: return to fertility and pregnancy risks after delivery; benefits of healthy spacing of pregnancy; contraceptive methods based on timing postpartum and breastfeeding status; benefits of exclusive breastfeeding including as a compoenent of the Lactational Amenorrhea Method (LAM) of contraception; and the need to transition to another modern method of contraception before LAM’s effectiveness wanes.
- Systematically offered information and services with the emphasis on integration of FP with other MNCH services for pregnant and postpartum women through a continuum of care.
- Implemented PPFP activities at community and facility levels, through high-quality service provision and social and behavior change communication, working closely with MNCH and nutrition providers and technical experts to refine strategies for effective integration of FP with other MNCH services.
- Fostered an enabling environment for PPFP at the national policy and health systems level.
- Advanced PPFP at the global level through strong advocacy and technical leadership, annual technical consultations, and ongoing working group activities in collaboration with global and field experts.
Over the years, and through effective collaboration across organizations, MCHIP-FP sought to raise awareness of the unique needs of women in the postpartum period and extending through two years after birth, as well as garnering momentum for addressing these needs through on-the-ground program implementation.
To learn more about MCHIP’s efforts to integrate FP along the MNCH continuum of care, click here.
Key Contributions to Family Planning
MCHIP invested in generating evidence on the practicalities and results of integrating FP within MNCH services. The following are highlights of field-based learning and subsequent resulting policy changes:
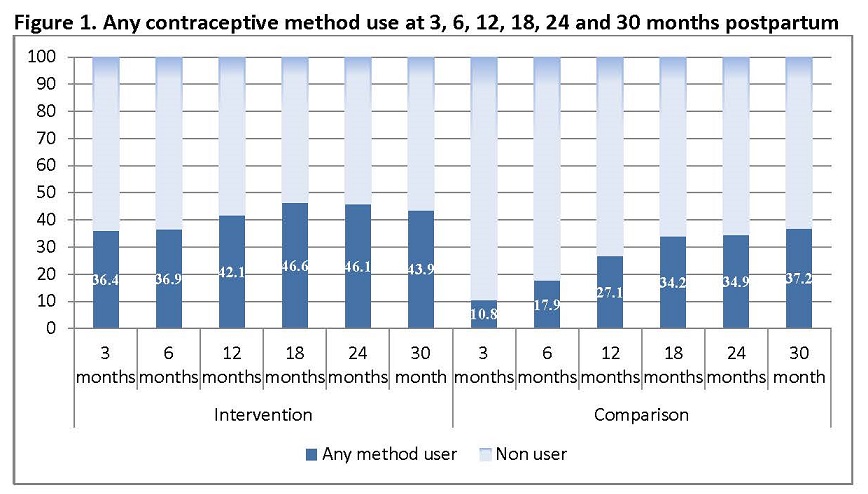
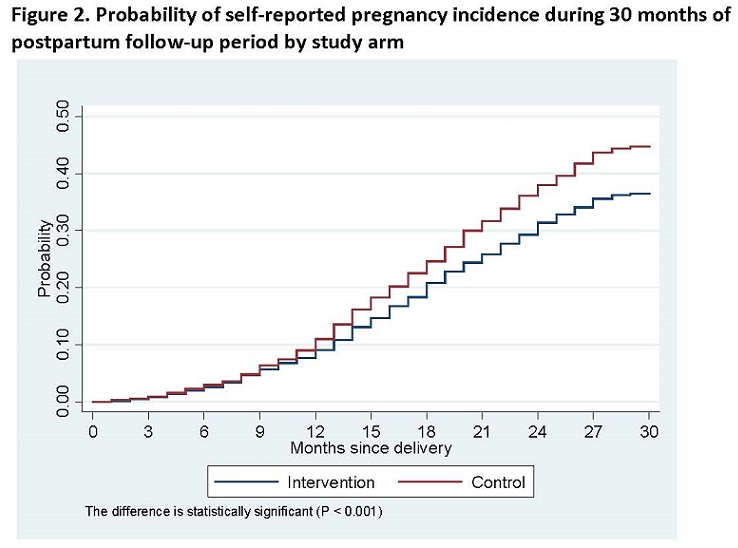
- Conducted the Healthy Fertility Study (HFS) in Bangladesh: MCHIP (previously ACCESS-FP), Johns Hopkins University Bloomberg School of Public Health, Shimantik, the Center for Data Processing and Analysis, and the Government of Bangladesh conducted an operations research study to examine the impact of FP integration on a community-based MNH program. Pre- and post-intervention surveys revealed that, when they reached 30 months postpartum, women who lived in communities where PPFP interventions were carried out were significantly more likely to use contraception (44%) than women in the same communities interviewed before the start of the PPFP activities (18%), and to initiate use of a method earlier than women in comparison communities. Figure 1presents postpartum contraceptive use among women with a surviving infant at 3, 6, 12, 18, 24 and 30 month’s follow-up. In both study arms, contraceptive use rates (any method) increased from 3, 6, 12, and 18 months postpartum but between 18 and 30 months contraceptive use rates in both arms stabilized and did not differ significantly. Overall, any method contraceptive use was higher among intervention area participants (n=904; 44%) as compared to those in the comparison arm (n=753; 37%). Furthermore, beyond the larger implications of increased early and sustained adoption of contraceptive use, the incidence of self-reported pregnancy and delivery was also considered. Figure 2shows the probability of becoming pregnant by 30 months was 44.8% in the control arm, compared to 36.5% in the intervention arm (p<0.001). Learning from the Healthy Fertility Study has influenced several at-scale programs in Bangladesh, including the MaMoni project.1
{kind=link}
{kind=link}
- Revitalized postpartum intrauterine devices as a vital postpartum FP method: Inspired by the success of colleagues in Paraguay,2 MCHIP developed learning resource materials for expanding access to this convenient method of PPFP. The article is based on a retrospective case series of over 3,000 postpartum IUD insertions. Findings from this study indicate that the expulsion rate for PPIUDs is much lower than reported in previously published literature. A plausible explanation for this is an improved clinical technique, and the same technique has been currently introduced in supported countries in Afghanistan, Ethiopia, Guinea, India, Mali, Mozambique, Pakistan, Philippines, Rwanda, Tanzania and Uganda. In particular, India is making great strides in scaling up services with strong leadership from the Ministry of Health and Family Welfare. Seventy-one hospitals and medical colleges in 19 states of India now offer the method to women who have given birth in facilities. A follow up study of a large cohort of Indian PPIUD acceptors also found a low expulsion rate. Furthermore, important policy changes have taken effect in India, for example to allow nurses and midwives to insert IUDs in the postpartum period, to engage dedicated PPFP counselors, and to target resources to six high priority focus States for further expansion of the services. As of May 2013, 100,000 women had received a PPIUD in India.
————-
1 The MaMoni project is a USAID associate award to the MCHIP Program, and is being implemented by Save the Children and two local nongovernmental organizations (Shimantik and FIVDB). It is an integrated safe motherhood, newborn care, and family planning project.
2 This work to be featured in a forthcoming issue of Contraception in a paper entitled “Postpartum Use of the Copper T 380A Intrauterine Device; The 10-year experience at Hospital Nacional, Asunción, Paraguay.”