Global Leadership
In 2011, USAID and MCHIP initiated a global call for action to promote and advance PPFP. This Statement for Collective Action for PPFP marked an important milestone for ACCESS-FP and MCHIP’s accomplishments in PPFP and was well-received by the international community. Notably, this statement was also endorsed by FIGO, the ICM, International Confederation of Nurses (ICN), AusAid, WHO/Reproductive Health and Research, UNFPA, International Planned Parenthood Federation (IPPF), World Bank, the Bill & Melinda Gates Foundation and various international NGOs.
A companion document released in 2013, called Programming Strategies for PPFP, was authored by WHO, USAID and MCHIP and represented the compilation of learning and contributions from a wide variety of experts and organizations that were consulted in its development. Short of a guidelines document, this resource for country programs offers useful suggestions for effective family planning integration with MNCH services.
MCHIP-FP supported several important areas of work and learning at the global level. These included: PPFP, lactational amenorrhea method (LAM) and transition, purposely testing promising models to integrate PPFP with MNCH service contacts, postpartum intrauterine contraceptive device (PPIUCD), and community-based PPFP. MCHIP-FP also co-led several working groups focused on learning about effective approaches to integration, including the FP/Immunization Integration Working Group, the Maternal, Infant and Young Child Nutrition FP (MIYCN-FP) Working Group, and the PPIUCD Working Group. These working groups not only generated interest in broader FP/MNCH integration, but accelerated the dissemination of learning from field applications and stimulate valuable exchanges amongst policymakers, implementing agencies, program managers and other stakeholders at the global and field level. Through the efforts of the FP/Immunization working group, a high impact practices brief was developed by USAID. The MIYCN-FP Working Group collaboratively produced a toolkit of resources, which was widely accessed. Lastly, MCHIP-FP facilitated online communities of practice around postpartum family planning. To become a member of the PPFP CoP, go to the PPFP Knowledge Gateway.
Program Learning Achievements
- Advocacy for Addressing Unmet Need for Postpartum Family Planning through Re-analysis of DHS Data: MCHIP-FP produced 10 descriptive country profiles focused on the extended postpartum period. These profiles demonstrate missed opportunities for integration of family planning by making use of existing DHS data for women two years postpartum. They also highlight unmet need for family planning, short birth-to-pregnancy and birth-to-birth intervals, timing of key factors related to fertility return, the relation of family planning use and relevant maternal newborn and child health care services, as well as contraceptive method mix. Traditionally unmet need for family planning is calculated by asking women if their current pregnancy or previous birth was wanted. However, in MCHIP’s re-analyses, unmet need is defined prospectively regarding the woman’s desired timing for her next pregnancy. Prospective unmet need is based on fertility preferences looking forward because it is most likely to predict a woman’s need for family planning in the extended postpartum period.
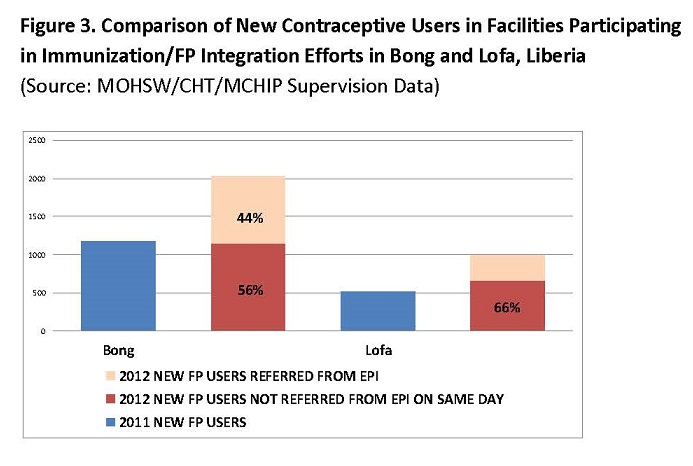
- Model Development in Integrated Service Delivery in Liberia: Beginning in 2011, MCHIP began a demonstration project to assess the feasibility and implications of integrating FP and immunization in a total of 10 facilities in Bong and Lofa counties. The model involved having vaccinators share brief family planning messages and referrals for same-day co-located FP services during routine immunization contacts at the health facilities. In March 2012, vaccinators, family planning providers, and supervisors were trained in integrated service delivery. Implementation of the integrated approach occurred over a period of 9 months, from March-November 2012. Endline results show 73% and 90% increases in new contraceptive users in each of the two counties, and the intervention did not appear to negatively affect immunization services. Figure 3 compares new contraceptive users in facilities participating in immunization/FP integration efforts in Bong and Lofa, Liberia.
- Model development in FP/MIYCN Integrated Service Delivery, Bondo, Kenya: In early 2011, MCHIP initiated an activity linking MIYCN and FP in Bondo District, in partnership with the Ministry of Public Health and Sanitation and other local stakeholders. By October 2011, an assessment had been completed, and subsequently, a MIYCN-FP training package for service providers and community health workers was prepared and the team conducted training for selected Community Health Workers and Facility-level service providers in June/July 2012. Implementation of the integrated approach was carried out in Bondo District Hospital, 5 other health facilities, and their adjacent community units.
{kind=link}
How did MCHIP Family Planning address equity?
The family planning team focused on the unmet needs of a particular group of women – those in the extended postpartum. In some countries, a further focus was on community-based programing where access to facility services is difficult, such as in Bangladesh, Afghanistan or Northern Nigeria. Lastly, each of the 10 PPFP country profiles included a disaggregated re-analysis of contraceptive use among women by wealth quintile, which has been used in country-level advocacy.
How did MCHIP Family Planning address scale?
The work of the MCHIP Family Planning team sought to keep the objective of achieving scale of evidence-based approaches in mind. Initial work was done on developing postpartum family planning integration scale-up readiness benchmarks. With a focus on understanding implementation modalities of various integration models, the downstream process of scaling up postpartum family planning took shape in selected field-supported programs and associate awards whose mandate includes scaling up, such as Bangladesh, India or Mozambique.
How did MCHIP Family Planning address community?
Given that social norms influence postpartum behaviors such as breastfeeding and use of health and family planning services, a focus of the MCHIP family planning work was on understanding barriers to adoption of family planning at that time. Strategies to overcome these barriers were developed and tested through community health worker platforms in a number of countries including Afghanistan, Bangladesh, Ethiopia, Kenya, Mali, Northern Nigeria, and to some extent Guinea. These activities looked not only at individual behaviors, but also at partner involvement, and building social/community support for PPFP through community mobilization and engagement of behavioral influencers such as religious and community leaders. Efforts to refine messages about return to fertility and facilitate behavior change also informed the learning agenda.
How did MCHIP Family Planning address quality?
MCHIP worked to ensure that programs and service providers understood the various contraceptive methods and their suitability based on timing postpartum and breastfeeding status. The MCHIP family planning program also worked to ensure that there were no missed opportunities in terms of maternal, newborn, child health contacts to offer protection against a closely spaced unplanned pregnancy. Furthermore, even while reinvigorating certain long-acting methods in the postpartum period, MCHIP always emphasized choice and voluntarism in its family planning programs and ensured compliance with US government regulations with respect to family planning programs.